Neurosurgery: Diagnostic and therapeutic modalities
Unique OCT probe with a 250μm package outer diameter, expect to be a LITT-compatible product system.
High-resolution and ultra-depth 1μm-6μm accuracy Guided LITT Probe Placement, compatible with intraoperative MRI guidance or without MRI guidance.
OCT probe capable of intraoperative real-time pathological evaluation of LITT ablation effect.
OCT probe Guided stereotactic biopsy needle capable of intraoperative real-time detection of cerebral vessels below millimeter level, which can completely avoid intraoperative complications of massive hemorrhage.
Imaging catheter compatible with neuro-intervention and Medtronic’s Pipeline Flex Shield stent, capable of real-time evaluation of preventing thrombotic complications.
NEUROSURGERY
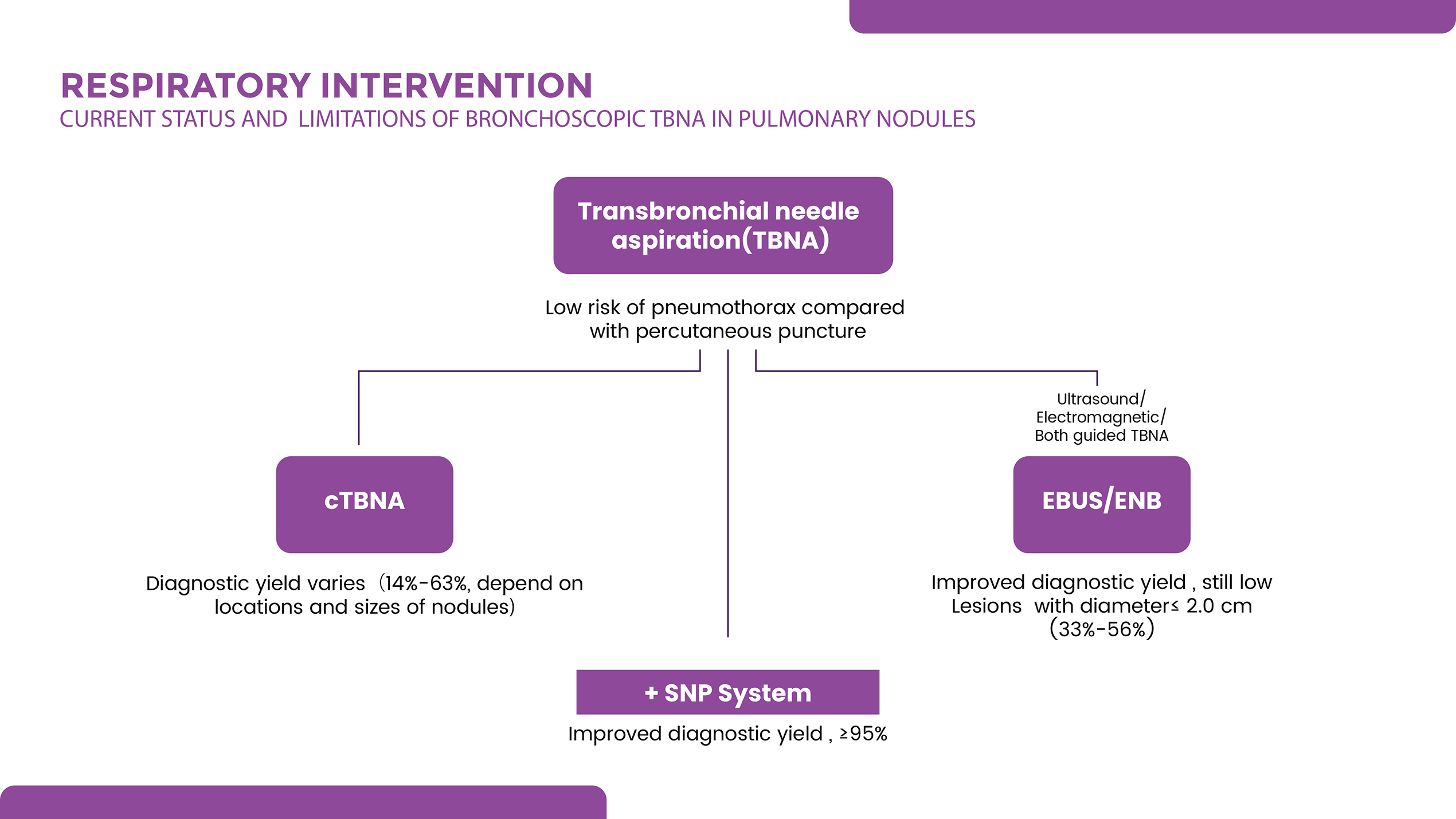
Respiratory intervention: patient needs
In 2015, 787,000 new cases of lung cancer surfaced across the world and it became the highest prevailing cancer with an average annual growth of 3.9%.
According to the RCT results of the National Lung Screening Test (NLST) in the United States, if lung cancer could be diagnosed early, followed by surgical resection of stage-IA or earlier lung cancer, the five-year survival rate was nearly 70%. However, the reality is that more than 75% of individuals are diagnosed with locally advanced or metastatic incurable lung cancer, for the first time, of which the five-year survival rate is less than 5%. So, the early and accurate diagnosis of lung cancer is key to the development of lung medicine.
According to NLST, after RCT of more than 50,000 participants, early diagnosis of lung cancer by low-dose spiral CT (LDCT) reduces the mortality rate by only 20% compared with standard chest X-ray. So, there is still controversy about the routine screening of lung cancer. And new technology to help early diagnosis of lung cancer becomes a significant need because an accurate diagnosis of a specific lung cancer type and stage is critical to determine optimal treatment. On the contrary, incorrect diagnosis may lead to inappropriate treatment and may result in life-threatening consequences.
The major progress of new technology in endoscopic imaging has brought great improvement to the staging and classification of early lung cancer. Developing guidance for airway biopsy to improve the biopsy diagnostic yield of early cancerous tissue is the key point.
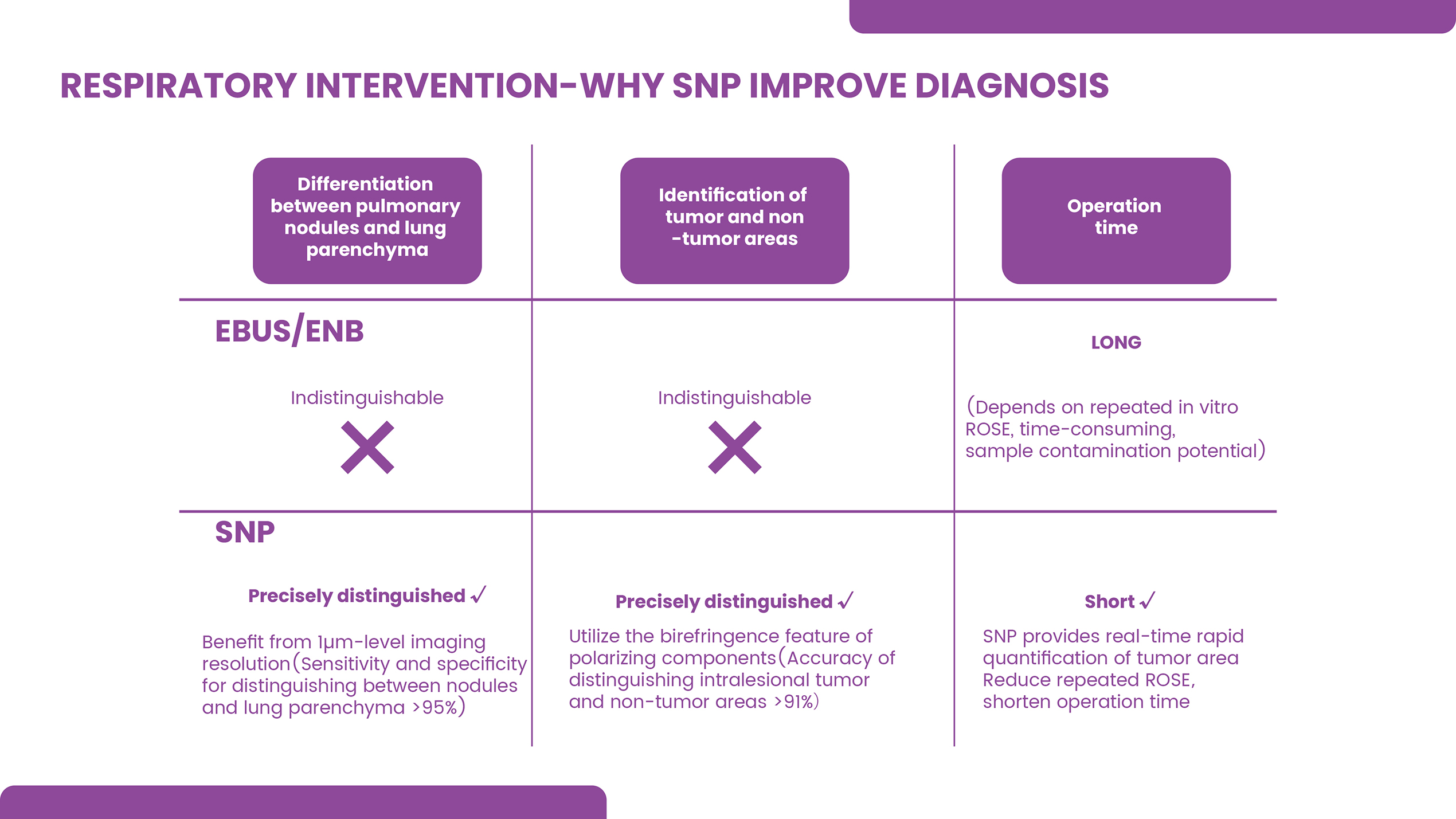
Since the penetration depth and resolution of various optical and acoustic techniques are significantly different, using multiple techniques with advantages in imaging depth or resolution respectively, for example, high-frequency endobronchial ultrasound (EBUS) capable of visualizing deep structures such as cartilage and potential tumor invasion, confocal laser endomicropy (CLE) with high-resolution that display microstructural changes, and ultrahigh-resolution ultrahigh-depth optical coherence tomography (OCT), become the future consensus on the clinical screening and diagnosis application in lung imaging.
Since the penetration depth and resolution of various optical and acoustic techniques are significantly different, using multiple techniques with advantages in imaging depth or resolution respectively, for example, high-frequency endobronchial ultrasound (EBUS) capable of visualizing deep structures such as cartilage and potential tumor invasion, confocal laser endomicropy (CLE) with high-resolution that display microstructural changes, and ultrahigh-resolution ultrahigh-depth optical coherence tomography (OCT), become the future consensus on the clinical screening and diagnosis application in lung imaging.
New Technology.
The major progress of new technology in endoscopic
The major progress of new technology in endoscopic imaging has brought great improvement to the staging and classification of early lung cancer. Developing guidance of airway biopsy to improve the biopsy diagnostic yield of early cancerous tissue is the key point.
The Cancer
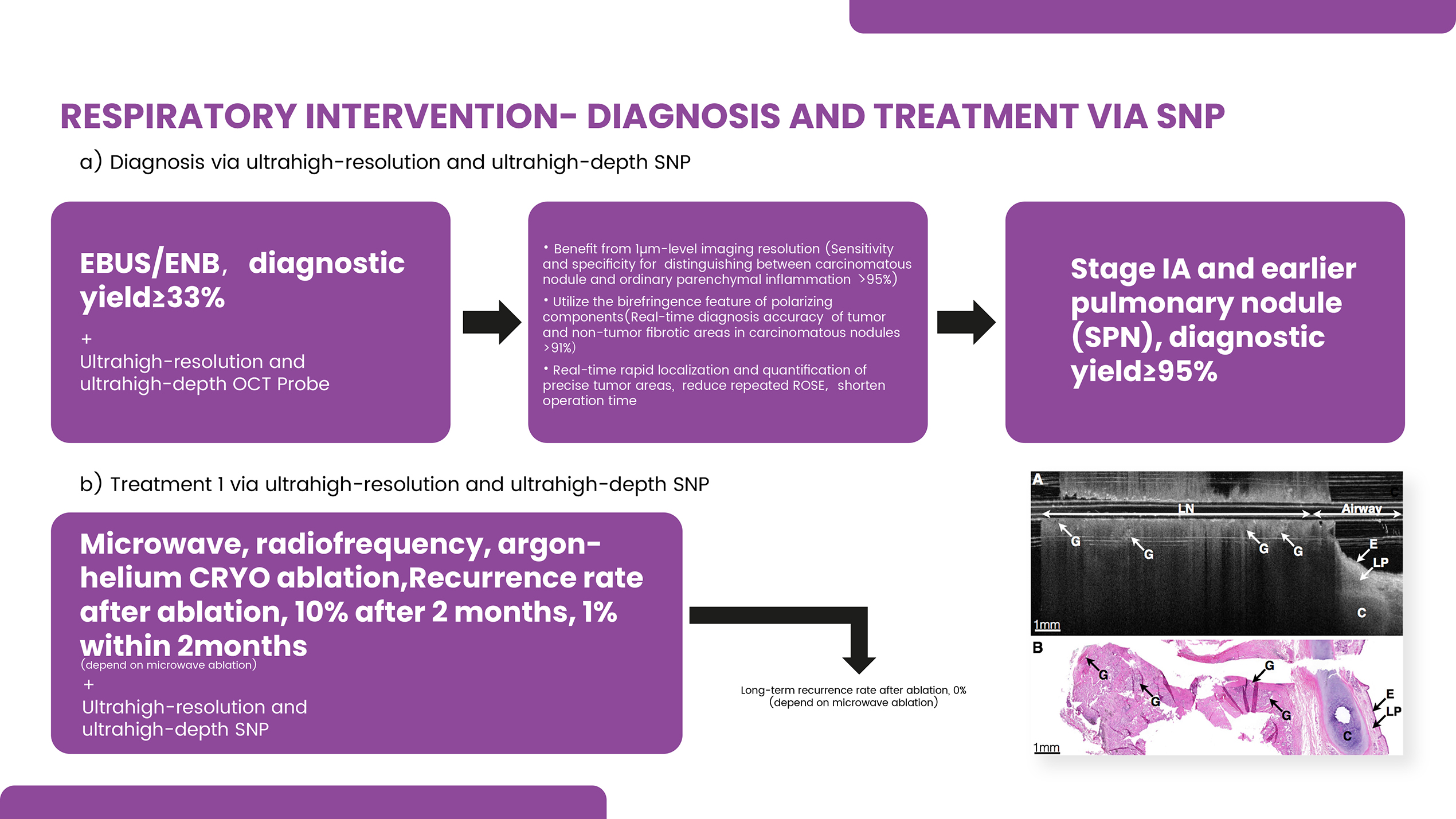
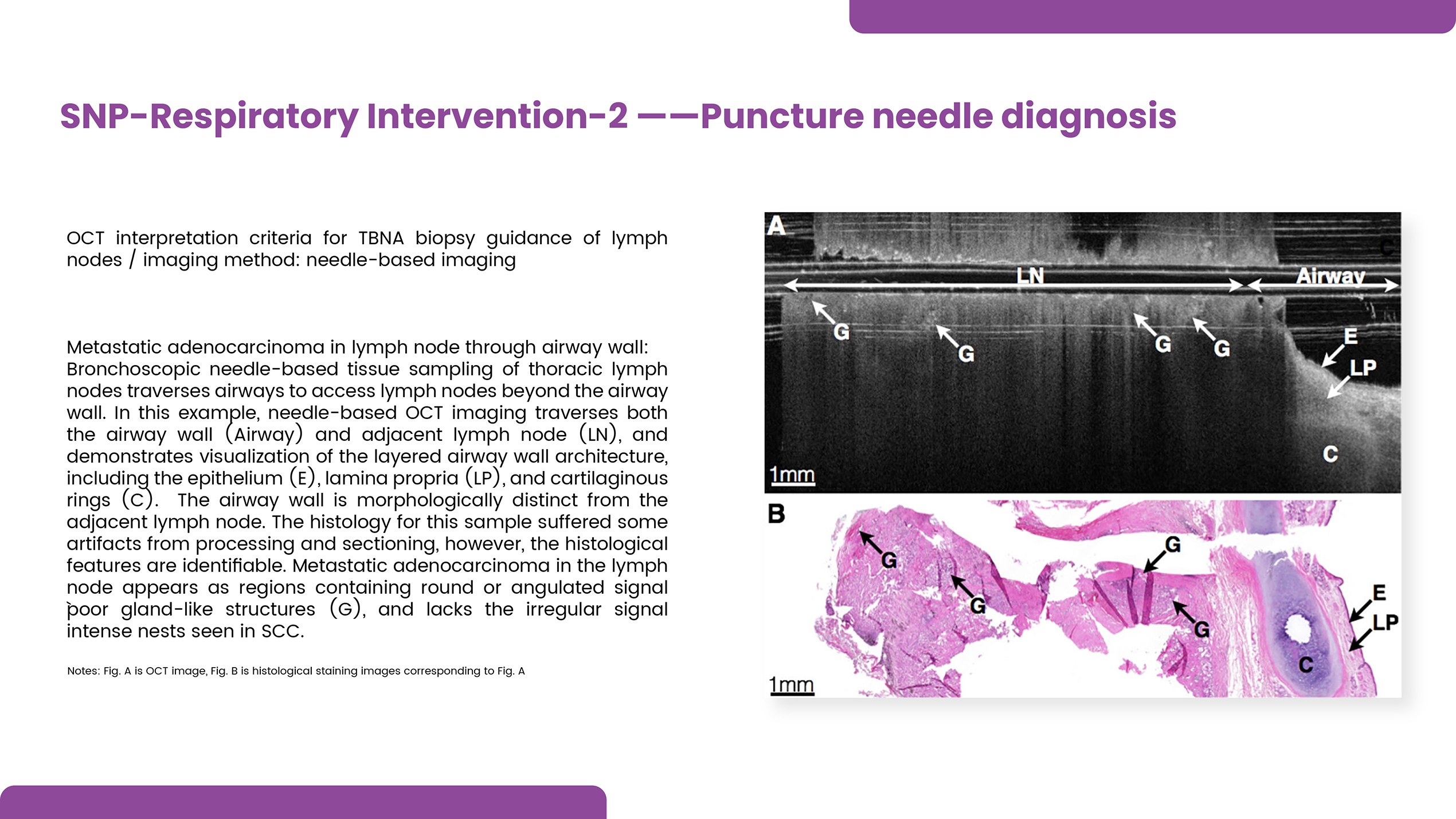
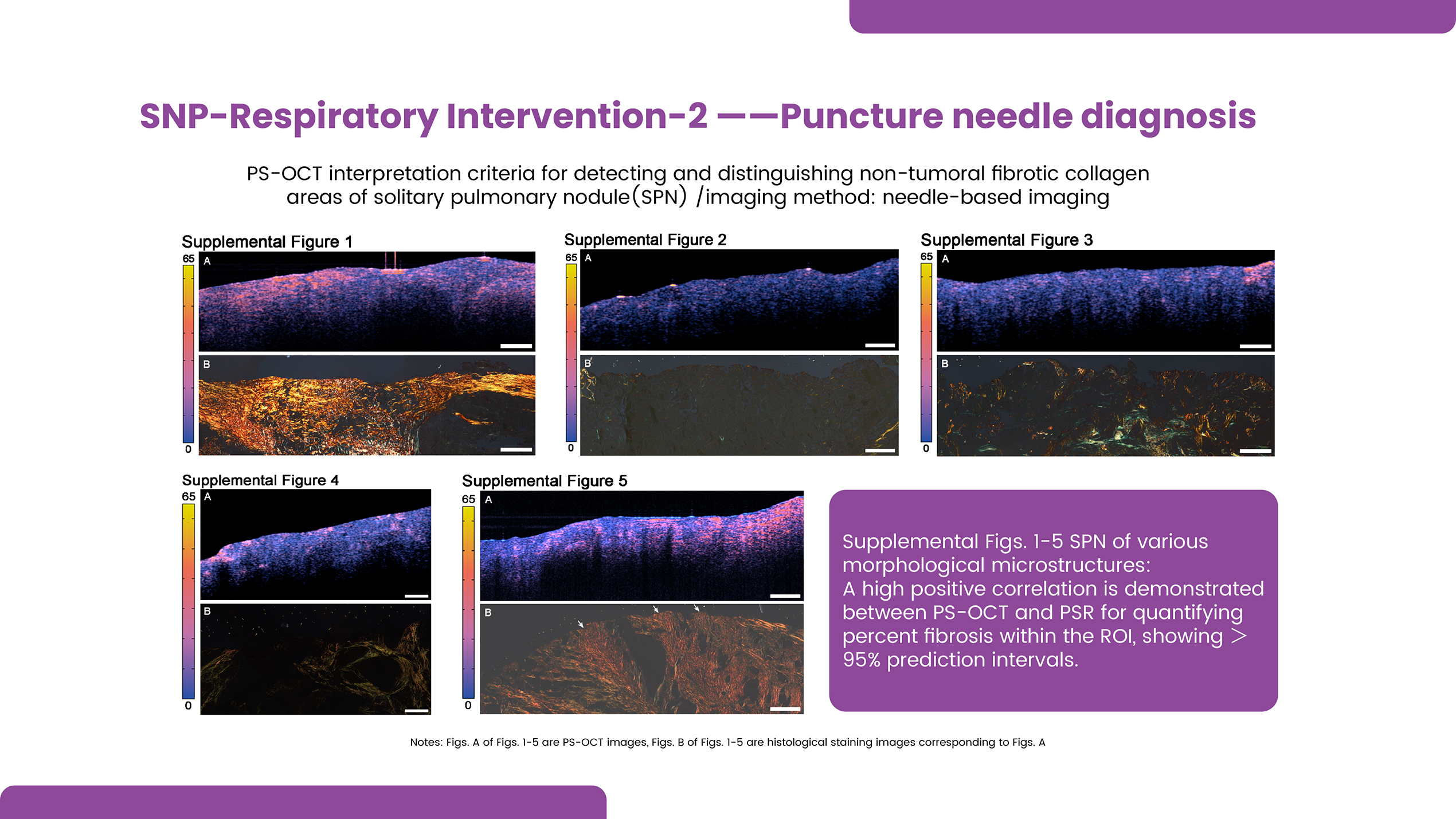
A Real-Time Deep Pathological Biopsy of Early Stage Lung Cancer
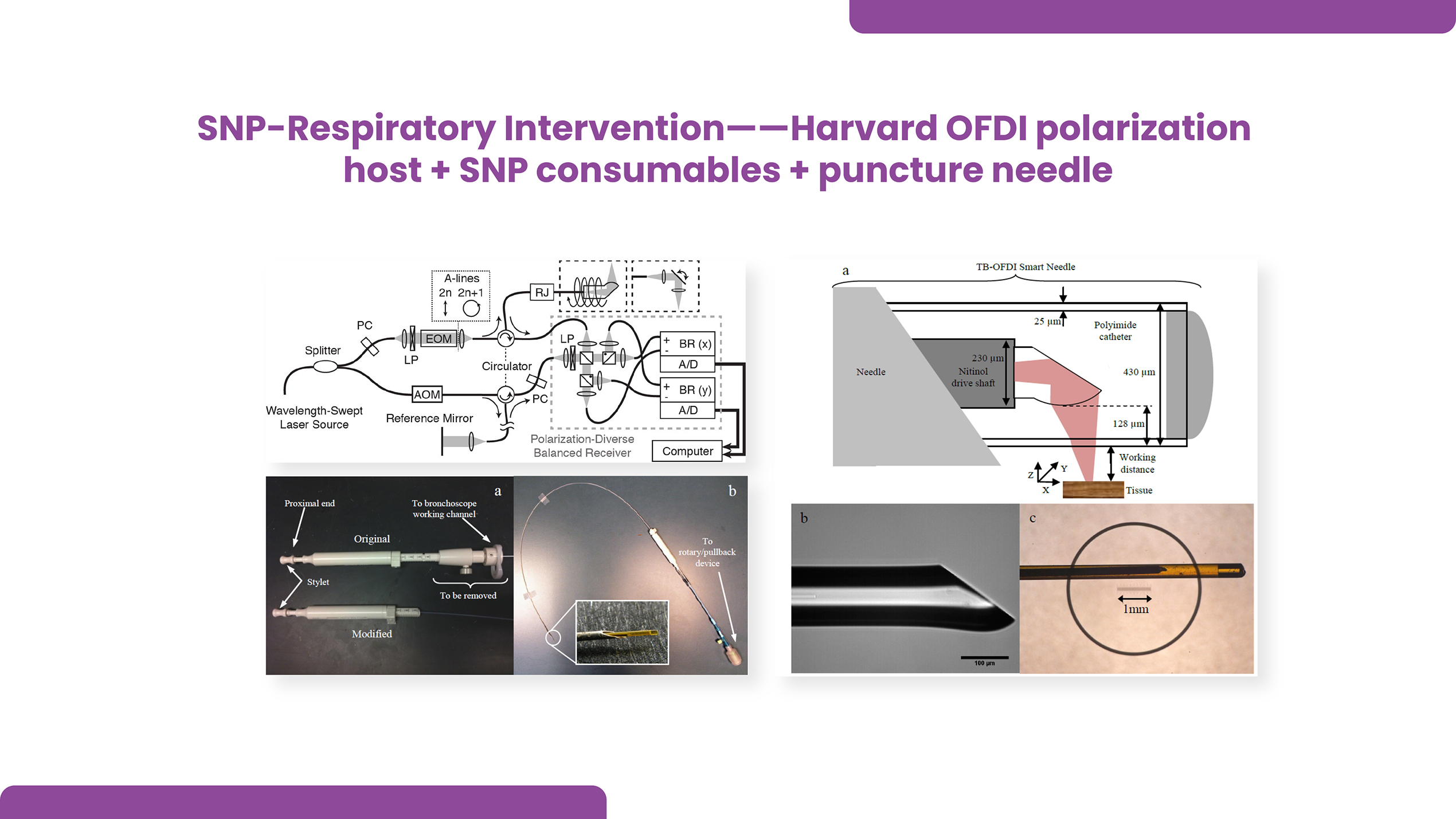
The only one who can perform real-time deep pathological biopsy of early stage lung cancer SPN (sole pulmonary nodule) (resolution: 900nm-1µm)
The only who has diagnostic consumables(diameter after encapsulation, down to 140µm) compatible with TBNA pinhole(inner diameter by 30G needle, down to 150µm ) .
The only one who can reach the imaging depth of 1cm-5cm, with a resolution 25 times that of ultrasound probes, and can completely replace the whole airway diagnostic technology and the thermal ablation margin evaluation diagnostic technology of the EBUS ultrasound probe.